Boutonnière deformity (also known as “buttonhole deformity”) is a condition that affects the fingers of the hand and directly impacts both their appearance and function. It most commonly occurs due to tendon injuries or inflammatory diseases such as rheumatoid arthritis, which lead to an imbalance in the movement of the finger’s middle joint (the proximal interphalangeal joint).As the condition progresses, a noticeable bending of the middle joint develops, along with difficulty in fully straightening the finger. This can cause both functional impairment and cosmetic concerns for the patient.Although the condition may appear mild in its early stages, neglecting it can lead to permanent finger deformity. Therefore, early diagnosis and appropriate treatment are essential for restoring normal hand function, we will explore everything related to Boutonnière deformity, including its causes, symptoms, diagnosis, treatment options, and prevention.
What is Boutonnière deformity?
Boutonnière deformity is an injury affecting the extensor tendon that runs over the middle joint of the finger (the central slip of the extensor tendon). This injury leads to tearing or weakening of the tendon, causing the middle joint of the finger to bend inward, while the tip joint becomes abnormally extended. This results in noticeable dysfunction of hand movement.
❓ Does Boutonnière deformity affect one finger or multiple fingers?
It usually affects a single finger, especially after a direct injury.
However, it may affect multiple fingers in chronic conditions such as rheumatoid arthritis.
❓ Can the deformity appear suddenly or develop gradually?
It may appear suddenly after a strong injury to the finger.
Or it may develop gradually over time in chronic conditions like rheumatoid arthritis.
❓ Can the condition be ignored if it is mild?
It is not recommended to ignore it even if it appears mild.
The condition may progressively worsen and lead to a permanent deformity if not treated properly.
❓ Does it affect the thumb?
It rarely affects the thumb.
It most commonly occurs in the other fingers such as the index, middle, and ring fingers.
❓ Is wearing a splint painful?
A splint is not inherently painful.
However, it may cause mild pressure or initial discomfort.
Despite that, it is an essential part of proper treatment.
❓ Can a person return to work or study during treatment?
Yes, in most cases the patient can continue work or study normally.
However, some adjustments may be needed to avoid putting pressure on the affected finger.
❓ Is surgery dangerous?
Surgery is generally not considered dangerous.
However, it requires high precision.
Post-operative physiotherapy is essential.
Results depend greatly on the severity of the condition before surgery.
❓ What happens if the condition is not treated?
The deformity may become permanent.
There will be reduced finger mobility.
Difficulty in gripping objects and performing daily activities may develop.
❓ Can the deformity return after treatment?
Recurrence is rare in most cases.
However, it may happen if:
- The underlying cause (injury or inflammation) recurs
- The patient does not follow medical instructions
❓ Does it affect writing or phone use?
Yes, especially in moderate or severe cases.
It reduces fine motor control of the finger, affecting precise tasks.
❓ Does it occur in children?
It is rare in children.
However, it may occur due to sports injuries or direct falls on the hand.
❓ Is the deformity painful?
It may be painful in the early stages, especially right after injury.
In chronic cases, pain may decrease while the deformity becomes more obvious.
Causes of Boutonnière Deformity
Boutonnière deformity occurs when the middle joint of the finger (PIP joint) bends inward, while the tip joint (DIP) extends outward. The main cause is damage or dysfunction of the central slip of the extensor tendon.
Main causes:
1) Rheumatoid arthritis
One of the most common causes.
Chronic inflammation gradually weakens the tendons and surrounding ligaments.
2) Direct injuries
Tearing or rupture of the central slip tendon.
A strong blow to the finger or sudden forced bending of the joint, often seen in sports injuries.
3) Cuts and trauma
Deep cuts on the back of the finger.
Fractures or dislocation of the proximal interphalangeal joint (PIP).
4) Burns and fibrosis
Burns may lead to scar tissue formation (fibrosis),
which disrupts tendon movement and balance.
5) Neglected minor injuries
Some injuries may seem minor at first,
but neglecting them can lead to worsening and eventual visible deformity over time.
Symptoms of Boutonnière Deformity
The symptoms of this deformity clearly affect both the appearance and function of the affected finger, and include the following:
1) Visible deformity of the finger
- Permanent or progressive bending of the proximal interphalangeal joint (PIP) inward.
- Hyperextension or outward bending of the distal interphalangeal joint (DIP).
- A characteristic “button-in-a-hole” appearance, which gives the condition its name.
2) Movement difficulty
- Reduced ability to fully straighten the PIP joint.
- Difficulty extending or controlling normal finger movement.
3) Pain and swelling
- Pain when moving the affected joint.
- Swelling around the PIP joint, more noticeable in inflammatory cases or recent injuries.
4) Joint stiffness
- Gradual stiffness of the joint.
- More noticeable in the morning or after periods of rest, especially in rheumatoid arthritis.
5) Functional impairment
- Difficulty performing fine motor tasks such as writing or buttoning clothes.
- Reduced hand strength in some cases.
Types of Boutonnière Deformity
Boutonnière deformity is not formally classified into strict medical types, but it is generally categorized based on stage, flexibility, or underlying cause.
First: Based on stage (most common classification)
1) Early (acute) stage
- The injury is recent.
- The PIP joint is still fully or partially extendable.
- Usually caused by a partial tear of the central slip tendon.
- Treatment is relatively simple, mainly splinting and physiotherapy.
2) Intermediate stage
- Progressive fixed flexion of the PIP joint begins.
- Clear difficulty in finger extension.
- Deformity becomes more visible during movement.
- Requires longer treatment and may not fully resolve without proper medical care.
3) Chronic stage
- The deformity becomes fixed and clearly visible.
- The PIP joint remains permanently flexed.
- DIP hyperextension becomes more pronounced.
- Often requires surgery or long-term rehabilitation.
Second: Based on correctability
1) Flexible (correctable) deformity
- The finger can still be manually extended or corrected with treatment.
- Tendons still retain some flexibility.
2) Fixed (non-correctable) deformity
- The joint becomes stiff.
- Fibrosis of ligaments and tissues occurs.
- Often requires surgical intervention.
Third: Based on cause
1) Rheumatoid deformity
- Caused by rheumatoid arthritis.
- Develops gradually over time.
2) Traumatic deformity
- Occurs after a direct injury to the finger.
- Such as tendon rupture, fracture, or dislocation.
Diagnosis of Boutonnière Deformity
Diagnosis mainly relies on clinical examination, with additional tests when needed.
1) Clinical examination (most important)
The doctor observes:
- Fixed or progressive flexion of the PIP joint.
- Hyperextension of the DIP joint.
- Difficulty or inability to fully extend the PIP joint.
Important test: Passive extension test
- If the joint can be manually extended → flexible, treatable conservatively.
- If it cannot be extended → chronic or stiff condition.
2) Medical history
Helps in diagnosis through:
- Previous finger injury.
- Presence of rheumatoid arthritis.
- Prior pain or swelling in the joint.
- Sudden or gradual symptom progression.
3) Functional assessment
- Measuring range of motion.
- Evaluating flexion and extension strength.
- Comparing with the healthy finger.
4) X-ray
Does not directly diagnose the deformity but is used to:
- Rule out fractures or dislocations.
- Assess joint changes, especially in rheumatoid arthritis.
- Evaluate joint erosion in chronic cases.
5) Additional tests (if needed)
- Rheumatoid factor tests (RF, Anti-CCP) if rheumatoid arthritis is suspected.
- MRI or ultrasound to assess the central slip tendon.
Complications of Boutonnière Deformity
Complications depend on severity, cause, and delay in treatment, ranging from mild symptoms to permanent deformity.
1) Permanent loss of finger function
- Inability to fully extend the PIP joint.
- Difficulty with fine tasks like writing or using a phone.
- Reduced hand strength, especially if multiple fingers are affected.
2) Joint stiffness
- Progressive loss of joint flexibility.
- Condition may become fixed and difficult to correct.
3) Permanent finger deformity
- Persistent PIP flexion.
- DIP hyperextension.
- Visible change in finger appearance.
4) Progression in chronic diseases
- In rheumatoid arthritis, other hand joints may also be affected.
- Leads to gradual functional decline if untreated.
5) Chronic pain
- Pain during movement or pressure.
- May become persistent in inflammatory cases.
6) Difficulty treating late cases
- Delayed treatment reduces chances of non-surgical correction.
- Advanced cases may require surgery or long-term rehabilitation.
Medical Treatment of Boutonnière Deformity (Medications)
Medication alone does not directly fix the deformity, because the main issue is tendon injury. However, drugs play an important role in reducing inflammation, relieving symptoms, and slowing progression.
First: Pain relievers and anti-inflammatory drugs
1) NSAIDs (Non-steroidal anti-inflammatory drugs)
Help to:
- Reduce pain
- Reduce swelling
- Reduce inflammation
Examples:
- Ibuprofen
- Diclofenac
- Naproxen
Notes:
- Do not repair the tendon injury
- Usually used short-term
- May cause stomach or kidney side effects with long use
2) Paracetamol (Acetaminophen)
- Used for pain relief only
- Does not reduce inflammation
- Preferred for mild cases or when NSAIDs cannot be used
Second: Corticosteroids
Used in severe inflammation or rheumatoid arthritis.
Forms:
- Oral tablets (e.g., Prednisolone)
- Local joint injections
Benefits:
- Rapid reduction of inflammation
- Decreases swelling in tendons and joints
Warnings:
- Not for long-term use
- May weaken tendons with prolonged use
Third: Disease-modifying drugs (for rheumatoid arthritis)
1) DMARDs
Examples:
- Methotrexate
- Hydroxychloroquine
- Sulfasalazine
Benefits:
- Slow or stop joint and tendon damage
- Prevent deformity progression
2) Biologic drugs
Used in advanced or resistant cases.
Examples:
- TNF inhibitors such as Etanercept and Adalimumab
Benefits:
- Precisely reduce immune system activity
- Significantly slow disease progression
Fourth: Supportive medications
- Vitamin D for bone health
- Calcium if needed
- Muscle relaxants in some cases
Important note
Medications cannot repair a torn tendon or correct finger shape.
However, they help to:
- Reduce inflammation
- Slow disease progression
- Protect other joints from damage
Surgical Treatment of Boutonnière Deformity
Surgery is indicated in Boutonnière deformity when the condition is chronic, fixed, or when conservative treatment (such as splinting and physiotherapy) fails. The goals of surgical intervention are:
- Restoring balance between the finger tendons
- Correcting flexion of the proximal interphalangeal joint (PIP)
- Improving hand function as much as possible, and sometimes appearance
First: Soft Tissue Release
These procedures are used in moderate or partially flexible cases.
1) Lateral band release
Concept:
Releasing the lateral bands that have shifted dorsally and contribute to PIP flexion.
Procedure:
- A small surgical incision is made on the back of the finger
- The lateral bands are released and repositioned
- They are fixed in the correct anatomical position
Goal:
- Restore extension of the PIP joint
2) Capsulotomy (joint capsule release)
Concept:
Used when there is joint stiffness or fibrosis.
Procedure:
- Opening the PIP joint capsule
- Removing adhesions and fibrotic tissue
- Restoring joint mobility as close to normal as possible
Second: Tendon Reconstruction
3) Central slip repair
Concept:
Repairing or reconstructing the damaged extensor tendon.
Procedure:
- Surgically exposing the tendon
- Suturing it if partially torn
- Using a tendon graft if necessary
4) Tendon transfer
Concept:
Using a healthy tendon to replace the damaged one.
Procedure:
- Harvesting part of a nearby healthy tendon
- Redirecting it to perform the function of the damaged tendon
- Fixing it to the PIP joint
Third: Tendon Balancing Procedures
5) Lateral band relocation
Concept:
Repositioning the lateral bands from the back to the front of the joint.
Procedure:
- Detaching the lateral bands
- Moving them to the anterior side of the joint
- Fixing them in place, usually with splint support after surgery
6) Tendon tightening or lengthening
Concept:
Adjusting tendon tension to restore balance between flexion and extension.
Fourth: Arthrodesis (Joint Fusion)
Used in severe or non-repairable cases.
7) Joint fusion
Procedure:
- Removing joint surfaces
- Fixing bones with screws or wires
Result:
- Complete loss of joint movement
- But a straight and more functional finger position
Fifth: Postoperative Care
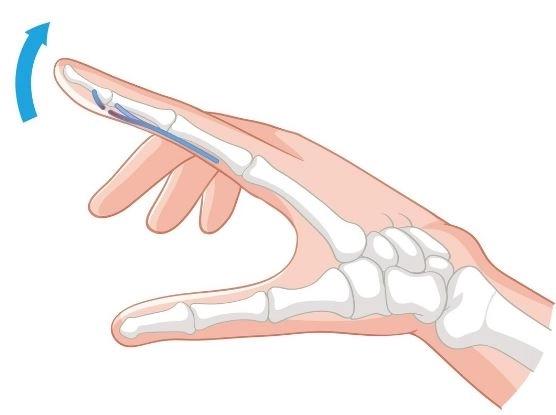
8) Splinting
- The PIP joint is immobilized in an extended position
- Usually for 4–6 weeks or longer depending on the case
9) Physiotherapy
- Prevents stiffness
- Gradually restores movement
- Strengthens tendons and surrounding muscles
Choosing the surgical method
| Condition |
Suitable surgery |
| Early and flexible |
Tendon repair + splinting |
| Moderate |
Soft tissue release + tendon repositioning |
| Chronic but mobile |
Tendon reconstruction |
| Severe and fixed |
Joint fusion |
Exercise Treatment for Boutonnière Deformity
Exercises are an important part of treatment, especially in early stages, after splint removal, or after surgery. However, exercises alone cannot repair a torn tendon. They help restore movement, prevent stiffness, and improve finger function.
Important before starting exercises
- In early cases, splinting in PIP extension is usually required
- Exercises should only begin after medical approval
Goals of therapy exercises
- Strengthen the central slip tendon
- Prevent stiffness of the PIP joint
- Improve finger range of motion
- Restore balance between PIP and DIP joints
Therapeutic exercises
1) Passive PIP extension
- Gently straighten the finger using the other hand
- Hold for 5–10 seconds
- Repeat 10–15 times, 3–5 times daily
Benefit: Prevents stiffness and improves flexibility
2) Isometric extension exercise
- Place finger on a flat surface
- Try to lift it slightly without strong movement
- Hold for 5 seconds
- Repeat 10 times, 2–3 times daily
Benefit: Strengthens extensor tendon safely
3) DIP flexion exercise
- Bend only the fingertip joint
- Keep PIP as straight as possible
Benefit: Restores tendon balance and reduces DIP hyperextension
4) Assisted extension
- Support finger movement using the other hand or elastic band
Benefit: Gradually improves range of motion
5) Light resistance exercise
- Use therapy putty or soft resistance bands
- Try to extend the finger against resistance
Benefit: Strengthens muscles and tendons
6) Stretching
- Gently extend the finger upward
- Hold for 15–30 seconds
- Repeat regularly
Benefit: Improves flexibility and reduces stiffness
Important guidelines
- Avoid strong pain or excessive force
- Progress gradually
- Stop if pain or swelling increases
- Consistency is more important than intensity
Duration of treatment
Usually 4–8 weeks or longer depending on severity
Best results occur when combined with splinting and physiotherapy
Prevention of Boutonnière Deformity
Prevention focuses on protecting the central slip tendon and avoiding injuries or conditions that weaken it.
First: Preventing injuries
1) Avoid direct finger trauma
- Be careful during sports like basketball, volleyball, and football
- Use protective equipment when needed
- Avoid forced bending of the finger backward
2) Use protective devices
- Finger splints during sports
- Buddy taping (taping fingers together)
- Protective gloves in contact sports
3) Proper handling of minor injuries
- Do not ignore finger pain or sprains
- Apply cold compresses in the first 24–48 hours
- See a doctor if symptoms persist
Second: Preventing complications after injury
4) Early treatment
- Immobilize the finger if tendon injury is suspected
- Use splints when necessary
- Follow treatment instructions carefully
Neglect is a major cause of permanent deformity.
5) Early physiotherapy
- Gentle exercises under supervision
- Maintain tendon flexibility
- Prevent joint stiffness
Third: Prevention in joint diseases (especially rheumatoid arthritis)
6) Control rheumatoid arthritis
- Follow prescribed medications (e.g., methotrexate)
- Regular medical follow-up
- Reduce inflammatory flare-ups
7) Reduce joint stress
- Use assistive tools to reduce hand strain
- Distribute pressure across the whole hand
Fourth: Daily preventive habits
8) Maintain finger flexibility
- Do light finger exercises daily
- Avoid prolonged finger flexion positions