

If you notice that your child suddenly starts limping or complaining of hip or knee pain without a clear reason, the issue may not be as simple as it seems. In some cases, this could be a sign of Perthes disease in children, a condition that affects the hip joint due to a temporary loss of blood supply to the head of the femur. Over time, this can weaken the bone and change its shape.Although the name may sound alarming, Perthes disease is not the end of the road. Most children improve significantly with early diagnosis and proper treatment, whether through physical therapy, medications, or sometimes surgery in more severe cases.In this article by Dleli Medical, we will explore Perthes disease in children, including its causes, symptoms, diagnostic methods, and the latest treatment options, so you can feel reassured and know how to respond from the very first warning sign.
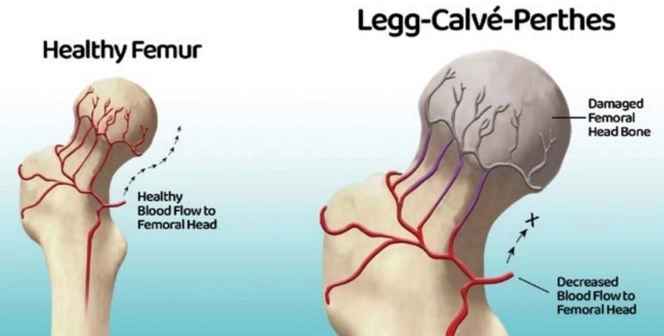
Perthes disease, also known as Legg-Calvé-Perthes disease, is a condition that affects the hip joint in children. It occurs when the blood supply to the head of the femur (the ball-shaped part that fits into the hip socket) is temporarily reduced or completely interrupted.
A healthy blood supply is essential for bones because it delivers oxygen and nutrients needed to maintain bone strength. When this blood flow decreases, the bone cells begin to die, a condition known as avascular necrosis.
As the lack of blood supply continues, the rounded head of the femur may gradually weaken, collapse, or change shape. Once blood flow returns, the bone starts rebuilding and strengthening itself again, but in some cases, the shape of the bone may remain permanently altered.
The severity of Perthes disease varies from one child to another. Some cases are mild, while others may be more complicated. However, early diagnosis and proper treatment play a major role in protecting the hip joint and reducing the risk of long-term complications.
Yes, many children recover well over time because the body gradually rebuilds the femoral head. The degree of recovery depends on several factors, including the child’s age, the severity of the condition, and how early treatment begins.
Treatment usually lasts between one and two years in mild to moderate cases. In more severe cases, recovery may take longer depending on the severity of the disease, the child’s age, and their response to treatment.
In most cases, Perthes disease does not lead to permanent disability, and many children are able to return to normal daily activities after treatment. However, advanced or untreated cases may lead to complications such as:
No, not every child with Perthes disease requires surgery. Many cases can be treated conservatively through:
Surgery is usually considered only in moderate to severe cases or when the hip joint does not respond well to conservative treatment.
That depends on the severity of the condition. Some children can walk relatively normally, while others may need:
Not all sports are prohibited, but high-impact activities are usually avoided temporarily, such as:
On the other hand, lighter activities such as swimming are often recommended because they help strengthen the muscles without putting pressure on the hip joint.
Perthes disease mainly affects children, but some of its long-term effects may continue into adulthood, including:
The exact cause of Perthes disease is still unknown. However, it appears more frequently in some families, suggesting that there may be a genetic factor that increases susceptibility, although it is not considered a directly inherited disease.
Yes, in some cases Perthes disease may cause a slight difference in leg length, especially if the condition significantly affects the growth of the femur. Usually, the difference is minor and does not cause major problems, but doctors monitor the child’s growth regularly to ensure healthy bone and joint development.
No, the pain is not always limited to the hip. Some children may complain of pain in the:
This can sometimes delay diagnosis because the underlying problem is actually in the hip joint, even though the pain appears elsewhere.
In most cases, Perthes disease does not return in the same hip after complete recovery, especially with proper treatment and follow-up. However, regular medical monitoring during growth remains important to ensure the hip joint develops normally and to detect any future complications early.
Perthes disease, medically known as Legg–Calvé–Perthes disease, progresses through several distinct stages. Each stage reflects the development of reduced blood supply to the femoral head and its effect on the hip joint.
At this stage, the blood supply to the femoral head begins to decrease.
During this stage, the blood supply becomes significantly reduced.
This is considered one of the most important and noticeable stages of the disease.
At this stage, the body gradually begins repairing the damaged bone.
In this final stage, the condition becomes stable.
Perthes disease, or Legg–Calvé–Perthes disease, is a condition affecting the hip joint in children. It occurs when blood flow to the femoral head decreases, causing the bone to weaken and change shape over time.
This is the primary cause. Insufficient blood reaches the femoral head, leading to gradual damage and weakening of bone cells.
Some children may have a family history of the condition, suggesting a possible inherited susceptibility.
Certain children may have weak or abnormal blood vessels supplying the hip joint.
Not usually one major injury, but repeated minor trauma to the hip may contribute to the disease in susceptible children.
The disease commonly appears between the ages of 4 and 10 years, a period of rapid growth that may be linked to its development.
Some studies suggest that exposure to cigarette smoke may affect blood circulation, although it is not considered a confirmed direct cause.
Symptoms of Perthes disease usually develop gradually and most commonly affect children between 4 and 10 years old.
This is often the first and most noticeable symptom. The child may begin walking abnormally or limping without a clear reason.
Pain may occur in the hip or thigh area. In some cases, the pain appears in the knee instead of the hip, which can delay diagnosis.
The child may avoid running or playing and become less active than usual.
There may be difficulty moving the leg or turning it outward, especially in younger children.
Parents may notice that the affected leg looks thinner or weaker than the other leg.
Pain often worsens during running or prolonged walking and improves with rest.
The diagnosis of Perthes disease, or Legg–Calvé–Perthes disease, depends mainly on physical examination and imaging tests because its symptoms may resemble other hip or knee conditions.
The doctor evaluates the child by:
Sometimes the child may complain only of knee pain, which can delay the diagnosis because the actual problem is in the hip.
X-rays are one of the most important diagnostic tools.
They can show:
However, in very early stages, X-rays may appear normal.
MRI helps detect the disease early before changes appear on regular X-rays. It can show:
Blood tests do not directly diagnose Perthes disease, but they help rule out other conditions such as:
Complications vary depending on the child’s age, the severity of the disease, and how early treatment begins.
The shape of the femoral head may become abnormal during the fragmentation stage, including:
This may affect hip joint movement later in life.
This is one of the most important long-term complications, especially if the femoral head does not heal into its normal shape.
It may increase the risk of developing early arthritis of the hip joint compared to healthy individuals.
A small difference in leg length may occur due to the effect of the disease on the growth of the femur on the affected side.
Children may experience:
In some severe cases, limping may continue even after the disease has completed its stages.
Because of reduced movement over a long period, the child may develop:
No, not all children develop complications. Recovery is usually better in younger children, especially with:
Treatment of Perthes disease, or Legg–Calvé–Perthes disease, with medications mainly focuses on relieving symptoms and improving the child’s comfort rather than directly treating the underlying cause.
The main problem in this disease is the reduced blood supply to the femoral head, so treatment usually depends on a combination of rest, physical therapy, and sometimes braces or surgery.
These are the most commonly used medications in children.
Common examples include:
Benefits include:
In some cases, muscle tightness may develop around the hip joint. Doctors may prescribe mild medications to help:
However, their use in children is usually limited and closely supervised by a doctor.
Doctors may sometimes recommend:
This is especially important if the child has nutritional deficiencies or weakened bones.
Currently, there is no medication that can directly restore blood flow to the femoral head or completely cure Perthes disease. However, ongoing research is exploring treatments that may improve bone nutrition and speed up recovery.
The child should avoid:
This helps protect the femoral head from deformity during the weakened stages of the disease.
Physical therapy is an essential part of treatment because it helps:
If the condition becomes advanced or significant bone deformity develops, the doctor may recommend:
Surgical treatment for Perthes disease, or Legg–Calvé–Perthes disease, is usually reserved for moderate to severe cases. The main goal of surgery is to keep the femoral head properly positioned inside the hip socket during healing and to reduce the risk of future deformities and complications.
Surgery is not always the first treatment option, but doctors may consider it when:
In this procedure, the surgeon makes a precise cut in the femur and changes its angle in order to:
This surgery reshapes or reorients the hip socket so it can better cover and protect the femoral head during healing.
In severe cases, surgeons may combine:
The goal is to achieve the best possible coverage and stability for the hip joint and improve the long-term outcome.
This procedure may be recommended when there is:
In cases where severe hip arthritis develops later in adulthood, the patient may require:
This procedure replaces the entire hip joint and is typically reserved for very advanced cases.
Recovery usually includes:
Recovery time depends on:
Specifically after surgery:
In many cases, yes — especially with:
However, some mild long-term effects may still remain, such as:






